

CMS Final Rule “Don’t Just Wait Until It’s Here”

As we discussed last week,
the CMS Final Rule on the elimination of “retroactive DIR fees” does not eliminate DIR fees, but rather eliminates the operative word “retroactive”. In other words, the lowest effective price will be reflected at the point of sale. Although this may help with budgeting and planning, it still does not correct the unfair and insufficient reimbursement that community-based pharmacists are currently experiencing. Community-based pharmacies must identify new opportunities for revenue generation beyond product distribution. This is no longer an option.
We all need to work diligently and deliberately to not only maximize current revenue opportunities (external to dispensing), but also identify newer opportunities that require investing time and resources to fully elucidate their potential. Below I am sharing revenue generating strategies we’ve initiated. These are not unique just to our practice, but rather are available to you and any community-based pharmacy practice that is ready and prepared to implement them.
Opportunity 1: Clinical Services
We have built the foundation of our practice on the development and implementation of clinical services (Figure 1 below). We have always maintained that our lowest hanging fruit for clinical services is a robust immunization service. Beyond the patient initial patient assessment to determine their eligibility and appropriateness for a vaccine, the process of administering the vaccine requires a short and defined time-period. Because of this, most vaccine programs can be done for a large number of patients during normal workflow. In addition, by utilizing technology and an online scheduling system (Figure 2 below), this can further improve efficiencies in vaccination services (and other offered services). Depending on the state you practice in, utilizing technicians as immunizers improves reach within the community by having more providers available to administer vaccines both within the practice and at remote sites. Our goal is to maximize all of our immunization opportunities.
Another clinical service we are maximizing is our medication management opportunities. This includes medication therapy management (MTM) opportunities with Medicare Part D, contracts with supported living community centers, long term care consulting, third-party payer programs (commercial, Medicare, and Medicaid), and our cash-paying patients. This means we need to be ready to provide the service at all times and ensure that the service is provided in a timely manner.
We have been involved in point-of-care testing since I came on board 16 years ago. It has grown from cholesterol, blood glucose, and A1c testing to COVID 19 testing to now statewide protocols for influenza and Strep A. These tests have been offered on a cash basi and provide a solution to the community-wide need of relatively quick, efficient, and affordable testing for patients.
One of our most robust services is our Medication Adherence Program (MAP). With this program, we work with older adults who have trouble managing their own medications. We assume total responsibility for their medications including medication reconciliation, refill services, medication reviews, and adherence packaging. We call our packaging service “Super Sync”. For a monthly service fee, patients receive these services routinely.
Opportunity 2: Cash-based practice
More recently we started a newer practice called Towncrest Wellness Apothecary (Figure 3 below https://www.facebook.com/towncrestpharmacy/) which is a cash-based practice only. It includes non-sterile compounding, a specialized negative pressure room for handling hazardous pharmaceutical powders, comprehensive options for quality supplements, CBD products, and specialized health and beauty aids. Functional medicine consults are provided for a fee. In the short time we’ve been open, we have seen a tremendous interest in growth in both compounding and functional medicine.
Opportunity 3: New business models
1. Direct contracting (Cost-Plus Model)
We have been working with two local businesses that came to us because of their concerns for their drug spend using one of the big three pharmacy benefit managers (PBMs). In both cases, the employer saved a tremendous amount of money, their employees and/or patients paid less out-of-pocket, and we were able to embed clinical services due to receiving a true professional fee with each dispensed medication. It truly has been a win-win-win for employer, patient, and pharmacy.
2. Concierge practice
We have had initial discussions with a physician who created his own concierge practice. He wanted to tap in on our clinical expertise as it relates to his patients’ medications. The initial discussions have centered on the services we provide to his patients, the monthly concierge fee we receive to provide those services, and how we can work collaboratively to ensure our mutual patients are achieving their therapeutic goals with safe and effective medications.
The challenge is to optimize all aspects of our practice including taking full advantage of all opportunities for non-dispensing revenue which includes payer programs, clinical services, participation in grants, and consulting revenue. It is equally important that we are maximizing our efficiencies with our dispensing functions by enrolling as many patients in our medication synchronization program as possible. We need to use our business acumen to ensure that we are getting the best cost-of-goods-sold, maximizing our wholesaler/buying group rebates, and managing our inventory, personnel, and expenses. Reviewing monthly financials and your cash flow frequently will help you make adjustments in your practice in a timely and effective manner.
The CMS final rule may be thought of as a small win for pharmacy, in terms of eliminating retroactive DIR fees, and now knowing at point of care the lowest effective price the pharmacy will receive. But the battle is far from over.
Product reimbursement will continue to be a struggle for community pharmacies and payer programs reimbursing for clinical services, though increasing, are still too few to offset the revenue lost from dispensing. This is why community-based pharmacy practices need to look for alternative revenue sources. The clinical services provided to your patients are not only a benefit to them, but it allows pharmacy staff to practice at the level of their training/education.
So, it’s a win-win—patients benefit and the practice benefits. As a wise pharmacist once said, “If it’s good for the patient, it’s good for the profession”. It is time for change!!
Figure 1

Figure 2
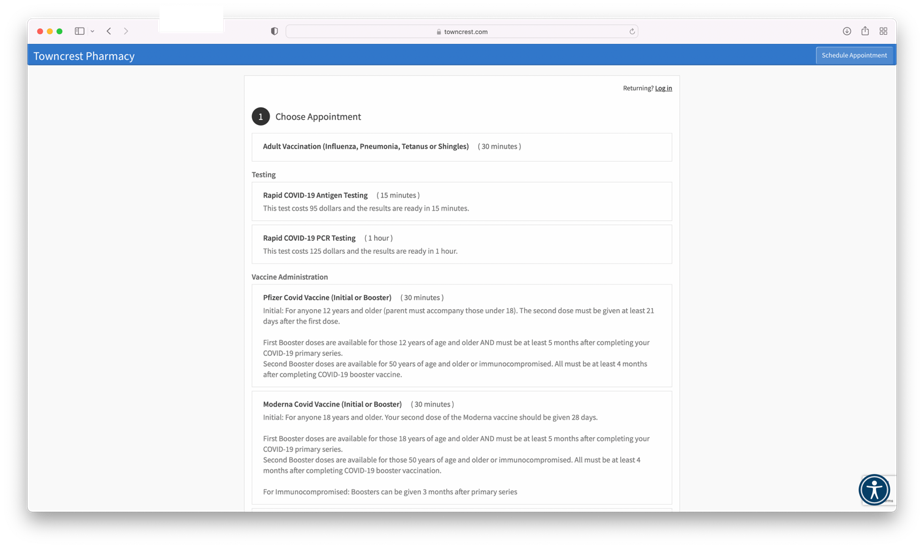
Figure 3
